Understanding the Upper Airway in Sleep Apnea
How Airway Collapse Occurs
Sleep apnea is a medically recognised sleep-related breathing disorder in which the upper airway repeatedly narrows or collapses during sleep, reducing or completely blocking airflow. In adults, the most common form is obstructive sleep apnea (OSA), where obstruction occurs at the level of the nose, soft palate, tonsils, tongue base, or throat.
During sleep, the muscles that support these soft tissues relax, and in susceptible individuals, this relaxation allows the airway to narrow significantly or collapse entirely for short periods. Each episode typically lasts at least 10 seconds and may occur repeatedly throughout the night, leading to drops in oxygen levels and fragmented sleep.
Structural Factors ENT Specialists Look For
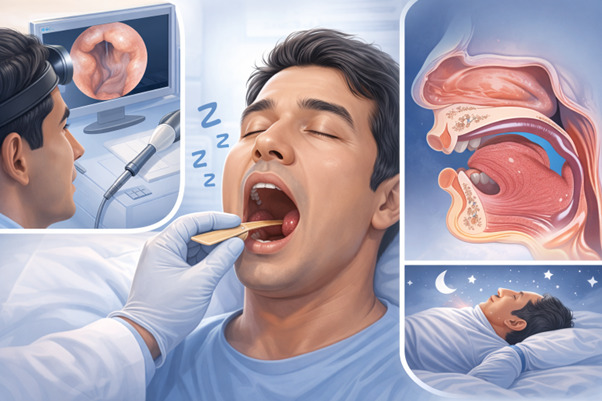
From an ENT perspective, anatomy plays a crucial role in symptom development. Enlarged tonsils, a long or bulky soft palate, a crowded tongue base, nasal septal deviation, and turbinate hypertrophy can all contribute to airway narrowing. Chronic nasal obstruction promotes mouth breathing, which further destabilises the upper airway during sleep. Careful examination of these structures allows the specialist to identify the mechanical factors that may be driving obstruction and to plan appropriate management.
Nocturnal Symptoms Commonly Reported

Loud, Persistent Snoring
Snoring occurs when airflow causes vibration of soft tissues in the throat. While simple snoring can occur without apnea, loud and disruptive snoring accompanied by irregular breathing patterns, choking sounds, or gasping raises concern for obstructive sleep apnea. Bed partners often report that the snoring is not only loud but also interrupted by worrying pauses.
Witnessed Breathing Pauses
A hallmark symptom of sleep apnea is the observed cessation of breathing during sleep. Partners may describe repeated episodes where breathing stops entirely, followed by a snort or gasp as airflow resumes. These events reflect airway collapse and the body’s reflexive effort to restore breathing. Many patients remain unaware of these episodes until they are highlighted by someone else.
Gasping, Choking, and Sudden Awakenings
Some individuals wake abruptly with a sensation of choking or struggling for air. These episodes may be mistaken for anxiety or reflux but frequently correspond to airway obstruction and oxygen fluctuation. Recurrent nightly episodes significantly disrupt restorative sleep and should not be ignored.
Restless and Fragmented Sleep
Sleep apnea causes repeated micro-arousals when the brain briefly activates to reopen the airway. Patients may toss and turn throughout the night and still wake feeling unrefreshed despite adequate hours in bed. Chronic fragmentation of sleep leads to cumulative sleep deprivation and persistent fatigue.
Nocturnal Mouth Breathing
Chronic mouth breathing during sleep is another important clue. Nasal obstruction due to septal deviation, allergic inflammation, or turbinate enlargement may predispose individuals to airway instability. Waking with a dry mouth or throat irritation is commonly associated with this pattern.
Daytime Symptoms With ENT Significance
Excessive Daytime Sleepiness
One of the most frequent complaints is overwhelming daytime fatigue. Patients may struggle to stay alert during routine activities because repeated airway obstruction prevents deep, consolidated sleep. This persistent sleepiness reflects disrupted sleep architecture rather than simple tiredness.
Morning Headaches
Morning headaches are a recognised symptom of obstructive sleep apnea. They are thought to be related to overnight fluctuations in oxygen and carbon dioxide levels. These headaches often improve as the day progresses but recur if the underlying breathing disorder remains untreated.
Dry Mouth and Throat Irritation
Persistent dryness or soreness on waking is commonly linked to overnight mouth breathing and snoring-related tissue vibration. Although seemingly minor, these symptoms often form part of a broader clinical picture.
Cognitive and Mood Changes
Poor concentration, memory lapses, and irritability are frequently reported. Chronic sleep disruption impairs cognitive performance and emotional regulation. Patients may attribute these changes to stress or ageing without recognising the role of a sleep disorder.
Subtle Signs Detected During ENT Evaluation
Chronic Nasal Obstruction
Long-standing nasal blockage increases airway resistance and may worsen snoring and apnea severity. Conditions such as septal deviation or turbinate enlargement contribute to this resistance. Addressing nasal factors can improve breathing dynamics and enhance tolerance to other therapies.
Enlarged Tonsils or Soft Tissue Crowding
In adults, enlarged tonsils or excess soft palate tissue can contribute to airway narrowing. A thickened or elongated soft palate increases the likelihood of collapse during muscle relaxation in sleep. Direct visual and endoscopic assessment helps determine the significance of these findings.
Tongue Base Contribution
The tongue plays a central role in maintaining airway patency. In some adults, the tongue base falls backwards during sleep and narrows the airway behind it. This mechanism may not be obvious without specialised evaluation.
Differentiating Sleep Apnea From Other Conditions
Not all snoring equates to obstructive sleep apnea. Some individuals have primary snoring without significant oxygen drops or repeated apnoeic events. Upper airway resistance syndrome may also cause sleep disruption without clearly defined apnea episodes. A thorough history, examination, and formal sleep study are essential for accurate diagnosis.
When to Seek Specialist Assessment
If loud snoring is accompanied by witnessed breathing pauses, choking episodes or excessive daytime sleepiness, specialist evaluation is advisable. Persistent morning headaches, unrefreshing sleep, and chronic nasal blockage are additional warning signs. Early consultation with an ENT specialist allows a detailed assessment of airway anatomy and appropriate investigation.
The Role of ENT in Treatment Planning
Treatment depends on severity and underlying anatomical factors. Continuous Positive Airway Pressure (CPAP) therapy remains a cornerstone for moderate to severe obstructive sleep apnea. ENT assessment helps identify structural contributors that may influence therapy selection or improve CPAP tolerance.
Tailored Management
Lifestyle optimisation, positional therapy, and oral appliances may benefit selected individuals. In cases of significant structural obstruction, surgical options may be discussed following a comprehensive evaluation. Conversations regarding sleep apnea treatment in Singapore typically involve a multidisciplinary approach to ensure individualised and evidence-based care.
Conclusion
Adult obstructive sleep apnea presents with a constellation of symptoms that extend well beyond simple snoring. Loud nocturnal breathing disturbances, witnessed apneas, gasping episodes, fragmented sleep, and persistent daytime fatigue are among the most common warning signs encountered in ENT practice.
Subtle anatomical contributors such as nasal obstruction, tonsillar enlargement, and tongue base crowding often underpin these symptoms. Early recognition and timely specialist assessment provide the opportunity for accurate diagnosis and effective treatment, ultimately improving sleep quality, cardiovascular health, and overall well-being.